Dilaudid vs Fentanyl: Clinical Comparison, Potency & Side Effects
Dilaudid (Hydromorphone) and Fentanyl (Sublimaze, Duragesic) sit at the absolute zenith of the American pharmaceutical analgesic ladder. These are not medications for 'everyday' pain; they are surgical and critical-care agents used when other high-potency narcotics have reached their limit.
- Dilaudid: A semi-synthetic opioid known for its rapid action and role as the 'rescue' drug of choice for acute trauma.
- Fentanyl: A fully synthetic opioid that is exponentially more powerful than almost any other substance, often used in microgram (mcg) doses.
In the U.S. clinical landscape, the difference between these two is a matter of scale—Fentanyl is roughly 25 times more potent than even the high-potency Dilaudid.

Dr. Kelsey Hopkins, MD
Dr. Hopkins practices rural family medicine in Southern Illinois, with a focus on community healthcare and chronic pain management.
Quick Reference Comparison
| Clinical Feature | Dilaudid | Fentanyl |
|---|---|---|
| U.S. Potency (MME) | 4.0 (Ultra-High) | 100.0 (Extreme) |
| Primary Formats | Tablets / IV | Patches / IV / Lozenges |
| Half-Life | 2 - 3 Hours | 7 - 24 Hours (Patch) / Short (IV) |
| Onset of Action | 15 - 30 Minutes | Seconds (IV) / Minutes (Spray) |
| Primary Use | Acute Severe Trauma | Chronic Cancer / Anesthesia |
Clinical Profile: Dilaudid

Dilaudid (Hydromorphone) is the 'heavy-hitter' of the pill world in U.S. medicine. Its profile is defined by:
- Rapid Brain Entry: Due to its chemical structure, it crosses into the central nervous system faster than Morphine or Oxycodone.
- The 'Hospital' Standard: It is the baseline for PCA (Patient-Controlled Analgesia) pumps in American recovery rooms.
- Renal Tolerance: Unlike many opioids, its metabolic byproducts are safer for U.S. patients with kidney issues.
While extremely powerful, it still functions conceptually like a 'stronger version of Morphine.'
Clinical Profile: Fentanyl
Fentanyl is a breakthrough in synthetic chemistry. In the U.S. healthcare system, it is categorized by:
- Micro-Dosing: It is so potent that it is measured in micrograms (mcg), not milligrams (mg). 100mcg of Fentanyl equals 10mg of Morphine.
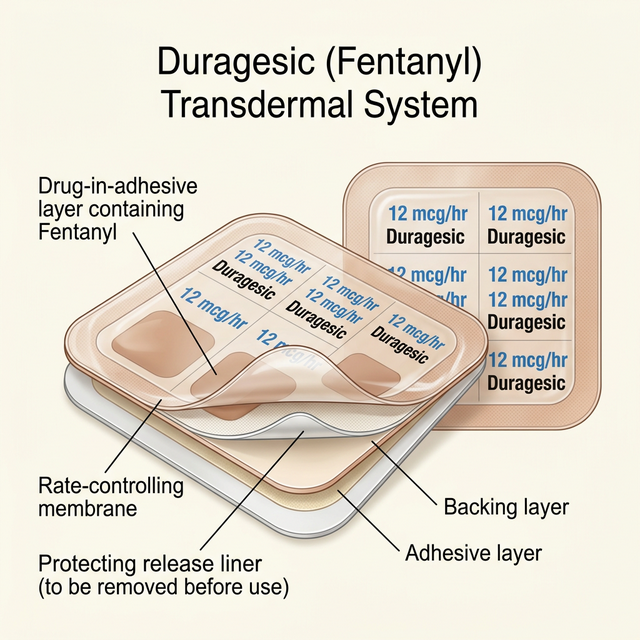
- Lipid Solubility: It is extremely fat-soluble, which is why it can be delivered through a skin patch (Duragesic) or a lozenge (Actiq).
- Short Duration (IV): In the OR, it is used for surgical maintenance because its effects wear off almost instantly once the drip stops.
Its potency is its greatest danger; even an amount the size of a few grains of salt can be lethal to an unsuspecting American patient.
Mechanism of Action: How They Work
Both target the 'Mu' opioid receptor, but their 'stickiness' and speed differ greatly:
- Dilaudid: Acts as a traditional pure agonist. It reaches its peak in the brain within 30-60 minutes when taken orally, providing a sharp relief peak.
- Fentanyl: Has an incredibly tight 'binding affinity.' Once it hits the receptor, it stays there with high intensity. Because it is so small and fat-soluble, it essentially 'leaks' through cell walls and into the brain faster than almost any other substance in the U.S. pharmacopeia.
Potency & Brain Absorption Scale
Direct Entry
Fentanyl crosses the brain barrier 10x faster than Dilaudid.
Potency Gap
Fentanyl is 25x stronger than Dilaudid milligram-for-milligram.
Lipid Path
Fentanyl can be absorbed through skin; Dilaudid cannot.
Receptor Lock
Fentanyl stays attached to pain sites with more 'grip'.
FDA-Approved vs. Off-Label Uses
Oversight by the U.S. FDA and clinical usage:
- Dilaudid FDA: Reserved for management of pain severe enough to require an opioid.
- Fentanyl FDA: Management of severe pain in *opioid-tolerant* patients (especially for the patch).
- Strict TIRF Program: Branded transmucosal fentanyl (Actiq, Fentora) is under a special U.S. FDA program called TIRF to prevent accidental death in non-tolerant patients.
Potency and Clinical Strength
Understanding the MME (Morphine Milligram Equivalent) Contrast:
- Dilaudid (4.0x): 2mg of Dilaudid = 8mg of Morphine.
- Fentanyl (100.0x): 2mg of Fentanyl = **200mg** of Morphine.
- The Ratio: Fentanyl is approximately **25 times more powerful** than Dilaudid. In most U.S. hospitals, if a patient is moved from one to the other, the calculation is done by multiple pharmacists to prevent a lethal error.
Bioavailability & Metabolism
Liver pathways and elimination for U.S. patients:
- Dilaudid: Metabolized via Glucuronidation. It is relatively 'friendly' to those on complex cocktail medications.
- Fentanyl: Heavily dependent on the **CYP3A4** enzyme. American patients must be warned that common items like grapefruit juice or certain antibiotics can 'clog' this enzyme, leading to a massive, fatal build-up of Fentanyl in their system.
Half-Life & Duration of Action
Duration of relief and stability:
- Dilaudid: Short half-life (2-3 hours). Effective relief lasts 3-4 hours.
- Fentanyl (IV): Ultra-short half-life (minutes). Great for surgeons.
- Fentanyl (Patch): Long half-life (72 hours). It releases a steady 'mist' of medication through the skin continuously.
Clinical Efficacy and Indications
U.S. Clinical Applications:
- The 'NPO' Patient: If a U.S. patient cannot swallow pills, the Fentanyl patch is the gold standard.
- Trauma/ER: IV Dilaudid is the preferred choice for immediate interception of severe pain.
- End-of-Life: Both are used, but Fentanyl is often preferred for 24-hours-a-day coverage without the need for frequent dosing.
Typical Dosage and Administration
Typical U.S. Dosing Strategies:
- Dilaudid: 2mg to 8mg tablets.
- Fentanyl Patch: 12mcg/hr to 100mcg/hr (replaced every 3 days).
- Important: A 'starting dose' of Fentanyl in the USA is only given to someone who has already been taking high doses of another opioid (like Dilaudid) for at least 7 days.
Side Effects and Adverse Reactions
Adverse reaction profiles for American patients:
- Respiratory Risk: Fentanyl is the most likely drug to cause 'Chest Wall Rigidity' (where you cannot breathe because your chest muscles freeze) if injected too fast.
- Itching: Fentanyl actually causes *less* itching than Dilaudid for many U.S. patients.
- Bradycardia: Fentanyl can slow the heart rate more significantly than Dilaudid.
Comprehensive Side Effect Analysis
| Adverse Event | Dilaudid (Potent) | Fentanyl (Extreme) |
|---|---|---|
| Slowed Breathing | Extremely High | CRITICAL |
| Heart Rate Slowing | Low | Moderate |
| Constipation | Very High | Extremely High |
| Itching (Pruritus) | Moderate | Very Low |
| Hallucinations | Moderate | High |
🔴 Dilaudid Risks
- Profound drowsiness
- Severe constipation
- Initial nausea
- Confusion in the elderly
- Dry mouth
🔴 Fentanyl Risks
- Lethargy / Brain fog
- Extreme constipation
- Nausea (especially during start)
- Dizziness
- Sweating
⚠ Critical Safety Note
Serious adverse reactions require immediate medical attention. The following are life-threatening signs:
- Fatal respiratory arrest (Breathing stops)
- Chest Wall Rigidity (Fentanyl IV)
- Severe hypotension (Low blood pressure)
- Fatal environmental interaction (Patch and heat/hot water)
- Serotonin Syndrome (at high doses)
Safety, Addiction Risk, and Controlled Status
⚠ U.S. Regulation: EXTREME (USA SCHEDULE II)
Safety and Regulatory Environment (USA):
- The 'Heat' Warning: American Fentanyl patch users are warned never to use a heating pad or sit in a hot tub, as heat causes the patch to dump a lethal amount of drug into the blood at once.
- Opioid Naivety: Giving Fentanyl to someone who hasn't been taking opioids is considered a 'Sentinel Event' (medical error likely to cause death) in U.S. hospitals.
- Diversion: Both are highly controlled; Fentanyl is the primary driver of the current illicit overdose crisis in the USA, although medical fentanyl is strictly tracked.
- Fentanyl: Dispose of used patches by folding them in half and flushing them—*never* throw them in the trash where a pet or child can find them.
- Dilaudid: Do not take for 'moderate' pain levels.
- Both: Zero alcohol; alcohol and Fentanyl is essentially a lethal injection.
- Keep Naloxone (Narcan) in the house; it is the only way to reverse an overdose of these powerful drugs.
Pharmacy Cost & U.S. Healthcare Access
Availability and U.S. Pricing:
- Dilaudid (Generic): Inexpensive ($20-$40).
- Fentanyl (Generic Patch): Expensive ($60-$150 per box).
- Fentanyl Branded (Actiq/Fentora): Extremely expensive ($500-$2,000+ per month).
Clinical Decision Flow: Which Should You Choose?
Clinical Decision Matrix for U.S. Physicians:
- Choose Dilaudid: For acute, severe 'rescue' need or for patients who need a highndpotency supplement to their daily meds.
- Choose Fentanyl: For long-term cancer pain, patients who cannot swallow, or those who need a constant, steady titration of the highest possible potency.
U.S. Ultra-Potency Selection Algorithm
Frequently Asked Questions
NEVER. In the U.S., it is a strict warning that cutting a patch can destroy the delivery membrane, causing all 72 hours of drug to release instantly into your blood.
While both are opioids, Fentanyl is synthetic and much more potent. 2mg of Fentanyl can be more lethal than 100mg of Heroin in many cases.
Because it is so powerful that even a single milligram (the size of a sugar grain) is too much for many patients. Micrograms allow for precision.
In the USA, this is a common 'breakthrough' strategy for cancer patients, but only under extremely strict oncological supervision.
With a patch, it can take 17-hours or more to clear the body even AFTER you take the patch off, because the drug stays in the skin's fat layers.