Understanding the Epidemic of Back Pain
In the United States, lower back pain is the leading cause of global disability and the most common reason for missed work. Modern American medicine categorizes back pain into three stages: Acute (less than 4 weeks), Subacute (4-12 weeks), and Chronic (over 12 weeks). Understanding your specific stage is critical for selecting the correct pharmacological and physical intervention.
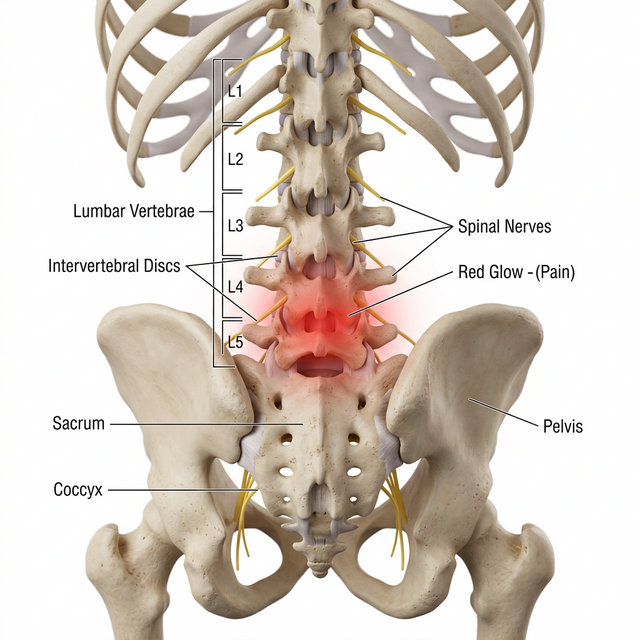
Clinical visualization of the lumbar spine and the neural architecture involved in chronic back pain signaling.
First-Line Clinical Interventions
According to the American College of Physicians (ACP), the first line of defense for non-radicular low back pain should focus on non-pharmacological treatments combined with simple analgesics.
| Treatment Class | U.S. Clinical Recommendation | Common Examples |
|---|---|---|
| Non-Steroidal (NSAIDs) | Primary for inflammation and acute strain. | Naproxen, Ibuprofen, Diclofenac |
| Muscle Relaxants | Short-term use (3-7 days) for acute spasms. | Cyclobenzaprine, Methocarbamol |
| Nerve Stabilizers | Used when pain radiates down the legs (Sciatica). | Gabapentin, Pregabalin |
| Physical Therapy | The "Gold Standard" for long-term recovery. | McKenzie Method, Core Stabilization |
The 'Active Recovery' Protocol
The paradigm of 'bed rest' has been clinically retired in the U.S. instead, physicians promote 'activity within limits.' This approach prevents the secondary complication of 'Fear-Avoidance,' where a patient's fear of movement leads to further muscular weakening and prolonged disability. Successful recovery programs often include:
- Dynamic Stretching: Gentle movements to maintain hip and spinal mobility.
- Core Integration: Strengthening the transverse abdominis to provide "internal bracing" for the spine.
- Aerobic Loading: Low-impact walking (15-30 minutes daily) to increase systemic circulation to spinal discs.
Chronic Back Pain & Central Sensitization
When back pain persists beyond three months, it often involves 'Central Sensitization'—a state where the nervous system remains in high alert even after the initial tissue injury has healed. In the U.S., managing this requires a multi-modal approach, often involving low-dose tricyclic antidepressants or SNRIs which block pain signals at the spinal cord level.
Frequently Asked Questions (Back Pain)
When should I see a doctor for back pain?
In the United States, 'Red Flags' requiring immediate urgent care include sudden loss of bowel or bladder control, severe leg weakness (foot drop), or pain that follows a major trauma like a car accident.
Is bed rest recommended for a thrown-out back?
No. Modern U.S. clinical guidelines strongly advise against bed rest for more than 24-48 hours. Movement, within a pain-safe range, promotes blood flow and faster healing of muscle fibers.
Do I need an MRI for simple lower back pain?
Most U.S. health insurance providers and medical boards recommend waiting 4-6 weeks before an MRI for uncomplicated back pain, as many issues resolve with conservative physical therapy.
What is the 'Active Recovery' model?
An American rehabilitative approach where patients engage in low-impact walking and core stability exercises early in the recovery phase to prevent muscle atrophy and chronic stiffness.
Is Heat or Ice better for a back spasm?
Typically, ice is used for the first 48 hours to reduce acute inflammation, followed by heat to relax muscle spasms and improve localized circulation.
Can stress cause back pain?
Yes. Psychological stress can lead to 'Muscle Guarding,' where the body subconsciously tightens the paraspinal muscles, creating a cycle of pain and tension commonly treated in U.S. pain clinics.
What are the most effective OTC meds for back pain?
NSAIDs like <Link href="/medications/naproxen">Naproxen (Aleve)</Link> often provide longer-lasting relief (up to 12 hours) than <Link href="/medications/ibuprofen">Ibuprofen</Link>, while <Link href="/medications/acetaminophen">Acetaminophen</Link> is preferred for those with sensitive stomachs.
What is a 'Slipped Disc'?
Clinically known as a herniated nucleus pulposus, it occurs when the soft center of a spinal disc pushes through a crack in the tougher exterior, often irritating nearby nerves.
When is surgery considered for back pain?
Surgery is generally the last resort in the U.S., considered only when neurological deficits (like numbness or weakness) progress or when 6-12 months of conservative therapy fails.
Are back braces helpful?
They can provide temporary support for acute injuries, but U.S. physical therapists warn that long-term use can weaken the core muscles, making the back more prone to future injury.
Clinical References
- American College of Physicians. (2025). Guidelines for Noninvasive Treatment of Low Back Pain.
- Journal of Bone and Joint Surgery. (2024). Herniated Discm Management in the USA.
- National Institute of Neurological Disorders and Stroke. (2026). Understanding Chronic Spinal Pain.