Fentanyl vs Dilaudid: Clinical Comparison, Potency & Side Effects

Fentanyl and Dilaudid (Hydromorphone) are two of the most powerful opioids available in the United States. They are typically reserved for patients who have 'failed' on Morphine or Oxycodone.
- Fentanyl: A purely synthetic molecule approximately 100x stronger than morphine.
- Dilaudid: A semi-synthetic derivative of morphine that is 5-7 times stronger than its parent molecule.
Both are Schedule II controlled substances and require expert management by U.S. pain specialists or hospital staff.

Dr. Kelsey Hopkins, MD
Dr. Hopkins practices rural family medicine in Southern Illinois, with a focus on community healthcare and chronic pain management.
Quick Reference Comparison
| Clinical Feature | Fentanyl | Dilaudid |
|---|---|---|
| U.S. Potency (vs Morphine) | 100.0 (Extreme) | 5.0 - 7.0 (High) |
| Drug Class | Pure Synthetic Phenylpiperidine | Semi-synthetic Hydrogenated Ketone |
| Common U.S. Form | 72-Hr Patch, IV, Lozenge | Tablets, Liquid, IV, Suppository |
| Histamine Release | Very Low | Moderate |
| DEA Schedule | Schedule II | Schedule II |
Clinical Profile: Fentanyl
Fentanyl is a highly lipophilic (fat-soluble) synthetic opioid. In American medicine:
- Surgery: It is the primary analgesic used in operating rooms for anesthesia.
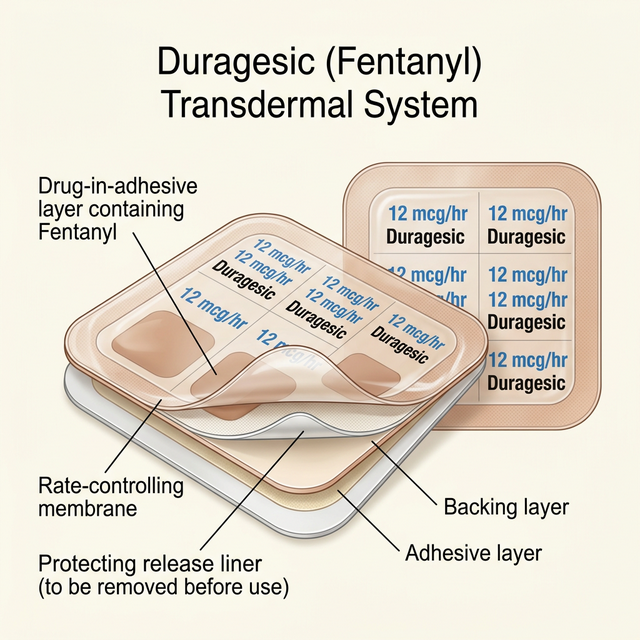
- Chronic Pain: The 72-hour patch (Duragesic) is the standard for steady-state relief.
- Safety: Reserved strictly for opioid-tolerant patients.
It acts instantly when injected but provides slow, steady relief when used as a patch in U.S. palliative care.
Clinical Profile: Dilaudid

Dilaudid is the brand name for Hydromorphone. In the U.S. medical system:
- ER Standard: Frequently used for acute traumatic pain (fractures, kidney stones).
- Potency: Often described as 'Morphine on Steroids' due to its high strength/low dose ratio.
- Solubility: Highly soluble, making it ideal for concentrated PCA (Patient Controlled Analgesia) pumps.
It is valued for having fewer side effects like itching compared to natural morphine.
Mechanism of Action: How They Work
Comparison of how these drugs interact with the Mu-Opioid receptor:
- Binding Affinity: Fentanyl binds extremely tightly, requiring higher doses of Narcan to reverse.
- Lipid Solubility: Fentanyl crosses the blood-brain barrier faster than Dilaudid.
- Metabolism: Fentanyl relies on CYP3A4; Dilaudid is processed via Glucuronidation (easier on the liver).
Receptor & Brain Entry
Lipid Entry
Fentanyl enters brain tissues faster than almost any other opioid.
Glucuronidation
Dilaudid metabolism bypasses the complex CYP pathway.
Histamine
Dilaudid causes more itching/flushing than Fentanyl.
MME Scale
1mg Dilaudid = 4mg Morphine; 1mg Fentanyl = 100mg Morphine.
FDA-Approved vs. Off-Label Uses
FDA-approved indications in the United States:
- Fentanyl: Chronic pain in tolerant patients and surgical anesthesia.
- Dilaudid: Management of severe pain where alternative treatments are inadequate.
- Off-Label: Both are used in U.S. hospice care for 'dyspnea' (shortness of breath).
Potency and Clinical Strength
The 20:1 Potency Ratio:
- Fentanyl (100x): The most powerful opioid in routine clinical use.
- Dilaudid (5x-7x): Significantly stronger than Morphine but weaker than Fentanyl.
- Equivalency: 1mg of IV Dilaudid is roughly equal to 20mcg of IV Fentanyl.
Bioavailability & Metabolism
- Fentanyl Bioavailability: High (92%) via patch or IV; low (30%) if swallowed.
- Dilaudid Bioavailability: Low (24%) via oral route due to heavy liver processing.
- Renal Safety: Both are considered safe options for American patients with kidney failure.
Half-Life & Duration of Action
- Fentanyl Duration: 72-hour steady delivery (Patch).
- Dilaudid Duration: Short (3-4 hours); typically requires dosing every 4-6 hours.
- Hospital Use: Dilaudid is preferred for 'prn' (as needed) breakthrough dosing.
Clinical Efficacy and Indications
Where they excel in U.S. clinics:
- Fentanyl: Best for stable, continuous chronic pain and hospice comfort.
- Dilaudid: Superior for acute 'spikes' of pain and PCA pump usage.
- Trauma: Dilaudid is the #1 choice for severe fractures in the USA.
Typical Dosage and Administration
- Dilaudid (Oral): Common doses are 2mg, 4mg, or 8mg tablets.
- Fentanyl (Patch): 12mcg/hr to 100mcg/hr dosages.
- Dilaudid (IV): Usually 0.2mg to 1.0mg per dose in U.S. emergency rooms.
Side Effects and Adverse Reactions
Adverse reaction comparison:
- Itching (Pruritus): More common with Dilaudid due to histamine release.
- Nausea: Both are high-risk; usually require anti-emetics in the USA.
- Chest Wall Rigidity: A unique risk of rapid IV Fentanyl injection.
Comprehensive Side Effect Analysis
| Adverse Event | Fentanyl (Synthetic) | Dilaudid (Semi-Synthetic) |
|---|---|---|
| Nausea / Vomiting | High | High |
| Itching / Hive-risk | Low | Moderate |
| Constipation | Very High | High |
| Sedation Level | Extreme | Severe |
| Breathing Depression | Extremely High | Extremely High |
🔴 Fentanyl Risks
- Severe Sedation ('The Nod')
- Patch site irritation
- Profound constipation
- Pinpoint pupils (Miosis)
- Confusion in elderly patients
🔴 Dilaudid Risks
- Moderate to severe itching
- Sudden dizziness (Orthostatic hypotension)
- Nausea and stomach cramping
- Dry mouth
- Urinary retention
⚠ Critical Safety Note
Serious adverse reactions require immediate medical attention. The following are life-threatening signs:
- Respiratory arrest (Fatal)
- Chest wall rigidity (Stiff Person Syndrome)
- Severe Hypotension (Blood pressure drop)
- Circulatory collapse
- Serotonin Syndrome when mixed with other meds
Safety, Addiction Risk, and Controlled Status
⚠ U.S. Regulation: EXTREME (USA SCHEDULE II)
Safety regulations and risks:
- DEA Schedule: Both are highly controlled with severe potential for abuse.
- Narcan Requirement: Stronger opioids often require multiple Narcan doses.
- Hospital Protocols: Dilaudid requires strict pulse-oximetry monitoring.
- Fentanyl: Avoid heating pads to prevent lethal dose dumping.
- Dilaudid: Do not combine with alcohol or sedatives (Xanax).
- Both: Use with extreme caution in sleep apnea patients.
- Keep emergency Narcan (Naloxone) in the household.
Pharmacy Cost & U.S. Healthcare Access
- Dilaudid: Generic Hydromorphone is inexpensive (approx $20/month).
- Fentanyl: Patches are more expensive ($60 - $120/month).
Clinical Decision Flow: Which Should You Choose?
Clinical decision-making in the United States:
- Choose Fentanyl: For long-term cancer pain or patients who can't swallow.
- Choose Dilaudid: For acute hospital trauma or short-term severe post-op pain.
U.S. Hospital Pain Protocol
Frequently Asked Questions
No. Fentanyl is 20 times more potent than Dilaudid milligram-for-milligram.
Yes, standard U.S. employment screens detect Hydromorphone as an opioid.
NEVER. Cutting a patch releases all the medicine at once, which is usually fatal.
Dilaudid is often preferred over Morphine in the elderly due to less metabolite buildup.
Yes, it typically causes more histamine release than purely synthetic Fentanyl.