Fentanyl vs Methadone: Clinical Comparison, Potency & Side Effects
Fentanyl and Methadone represent the 'Apex' of synthetic opioid pharmacology in the United States. While both are strictly regulated Schedule II substances, they function on fundamentally different biological clocks and molecular pathways.
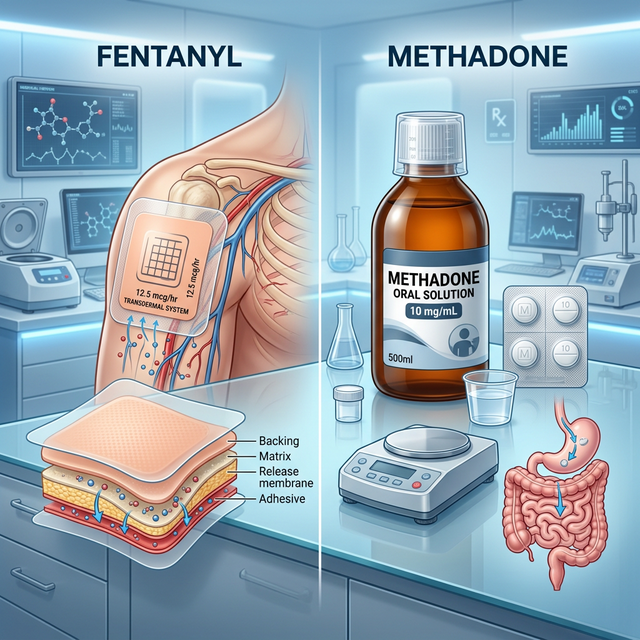
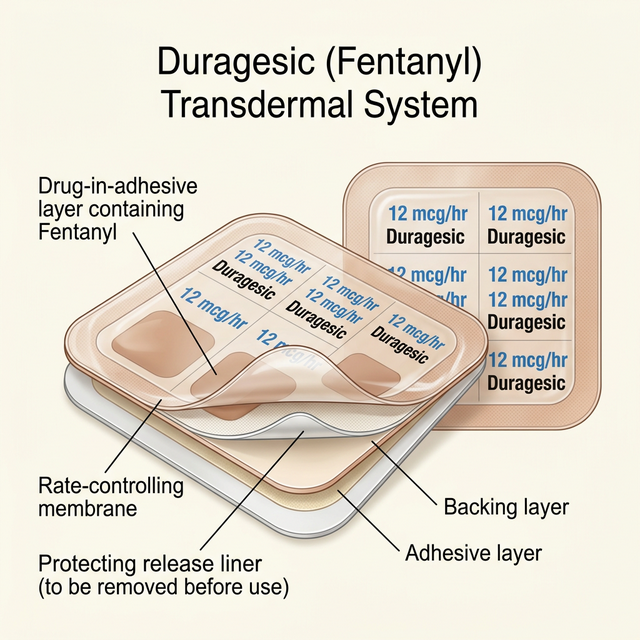
- Fentanyl: A lipophilic powerhouse designed for rapid, steady-state delivery via transdermal patches or transmucosal products.
- Methadone: A complex pharmacological agent that targets both opioid and NMDA receptors, offering unique dual-action relief.
This guide analyzes the performance, safety profiles, and clinical trade-offs of these two potent medications within the American healthcare system.

Dr. Kelsey Hopkins, MD
Dr. Hopkins practices rural family medicine in Southern Illinois, with a focus on community healthcare and chronic pain management.
Quick Reference Comparison
| Clinical Feature | Fentanyl | Methadone |
|---|---|---|
| U.S. DEA Status | Schedule II Controlled | Schedule II Controlled |
| Primary Target | Mu-Opioid Receptors | Mu-Opioid + NMDA Antagonist |
| MME Conversion | 72x - 100x Morphine | 3x - 12x (Variable) |
| Cardiac Risk | Minimal / Negligible | High (QT Prolongation) |
| Half-Life | 3-7 hours (Effective) | 8-59 hours (Accumulative) |
| Metabolism | CYP3A4 Pathway | CYP3A4, 2B6, 2C19 |
Clinical Profile: Fentanyl
Fentanyl is a high-potency synthetic opioid 100 times stronger than morphine. Key characteristics include:
- Rapid Delivery: Crosses the blood-brain barrier almost instantly due to high lipid solubility.
- Versatile Forms: Available as 72-hour patches (Duragesic), lozenges (Actiq), and IV formulations.
- Microgram Dosing: Precisely measured in mcg, not mg, due to its extreme potency.
In the USA, it is the 'Gold Standard' for surgical anesthesia and managing intractable breakthrough cancer pain.
Clinical Profile: Methadone

Methadone is a dual-action synthetic opioid used for both chronic pain and addiction. Unique clinical features include:
- NMDA Antagonism: Blocks the receptors responsible for nerve pain and opioid tolerance.
- Extreme Half-Life: Stays in the blood for up to 60 hours, leading to significant accumulation risk.
- Low Cost: One of the most affordable long-acting opioids in the United States.
While often associated with clinics, it is a powerhouse tool for 'refractory' pain cases that fail standard narcotics.
Mechanism of Action: How They Work
How do these molecules interact with the human nervous system?
- Fentanyl: Acts as a 'Pure Agonist' at the Mu-Opioid receptor, effectively dampening sensory perception of pain.
- Methadone: Functions as a Mu-Agonist while simultaneously blocking NMDA receptors and inhibiting serotonin/norepinephrine reuptake.
- Therapeutic Focus: Fentanyl is a 'blanket' block; Methadone is a 'precision' reset of over-excited pain nerves.
Receptor Activity Comparison
Mu-Opioid
Primary target for both drugs to achieve pain relief.
NMDA Block
Only Methadone resets excited nerve pathways.
CYP3A4
Primary metabolic engine for both synthetic opioids.
hERG Channel
Methadone interacts here, affecting heart rhythm.
FDA-Approved vs. Off-Label Uses
Understanding FDA oversight in the American medical system:
- Fentanyl FDA Uses: Management of severe chronic pain in opioid-tolerant patients only.
- Fentanyl Prohibitions: NOT approved for acute pain, opioid-naive patients, or minor surgeries.
- Methadone FDA Uses: Moderate-to-severe chronic pain and opioid detoxification/maintenance.
- Off-Label Use: Refractory Restless Leg Syndrome (RLS) and terminal respiratory distress.
Potency and Clinical Strength
Comparison of potency levels using the U.S. MME standard:
- Fentanyl Strength: 100x stronger than Morphine; typically measured in mcg (micrograms).
- Methadone Strength: Variable; potency increases exponentially as the dose rises.
- The Conversion Rule: Fentanyl conversions are linear; Methadone conversions require a sliding scale.
Bioavailability & Metabolism
- Fentanyl Patch: 92% bioavailability; bypasses the liver's 'first pass' effect.
- Methadone Tablet: 80% bioavailability; requires multiple digestive pathways.
- Liver Clearance: Both rely heavily on the CYP3A4 enzyme for detoxification.
Half-Life & Duration of Action
- Fentanyl: Effective half-life is managed by the 72-hour patch reservoir.
- Methadone: Unpredictable half-life (8-59 hours), leading to drug stacking.
- Safety Limit: Methadone should never be dose-adjusted more than once a week.
Clinical Efficacy and Indications
Clinical efficacy comparison in American studies:
- Fentanyl: Superior for end-stage cancer pain and surgical sedation.
- Methadone: Gold standard for neuropathic (nerve) pain and opioid-induced hyperalgesia.
- Preference: Doctors prefer Fentanyl for simplicity; Methadone for complex nerve syndrome.
Typical Dosage and Administration
- Fentanyl: 12mcg/hr to 100mcg/hr patches, changed every 3 days.
- Methadone: 2.5mg to 10mg started usually 3 times daily.
- Dose Ramping: Methadone requires 'Start Low, Go Slow' protocol over 5-7 days.
Side Effects and Adverse Reactions
Key side effect trade-offs in the USA:
- Constipation: Generally more severe with 24/7 Fentanyl patch coverage.
- Sweating: Significantly more common with long-term Methadone use.
- Heart Safety: Only Methadone carries a risk for QT prolongation.
Comprehensive Side Effect Analysis
| Adverse Event | Fentanyl (Patch) | Methadone (Oral) |
|---|---|---|
| Stomach Distress | Extremely High | High |
| Cardiac Impact | Negligible | High (Requires EKG) |
| Accumulation Risk | Low | Extremely High |
| Skin Reactivity | High (Adhesive) | None |
| Night Sweats | Low | Very High |
🔴 Fentanyl Risks
- Severe Sedation / 'Nodding'
- Itching / Skin Rash at site
- Nausea and Vomiting
- Profound Narcotic Constipation
- Chronic Dry Mouth
🔴 Methadone Risks
- Excessive Sweating (Hyperhidrosis)
- Step-like Sedation (Cumulative)
- Dizziness and Lightheadedness
- Peripheral Edema (Leg Swelling)
- Weight Gain
⚠ Critical Safety Note
Serious adverse reactions require immediate medical attention. The following are life-threatening signs:
- Respiratory Depression (Fatal breathing stop)
- QT Prolongation / Sudden Cardiac Arrest (Methadone)
- Heat-Induced Patch Overdose (Fentanyl)
- Lethal Drug Accumulation (Day 4-5 danger)
- Serotonin Syndrome with SSRIs
Safety, Addiction Risk, and Controlled Status
⚠ U.S. Regulation: EXTREME (DEA SCHEDULE II)
Safety considerations for high-potency opioids:
- Addiction Risk: Both have high potential for physical and psychological dependence.
- The Heat Rule: Hot tubs or heating pads can trigger a lethal Fentanyl dump.
- EKG Monitoring: Mandatory for Methadone to prevent silent heart failure.
- Withdrawal: Methadone withdrawal is notoriously long (up to 6 weeks).
- Never use heating pads on a Fentanyl patch site.
- Methadone requires a baseline EKG for heart safety.
- Avoid alcohol and benzodiazepines with both medications.
- Keep Naloxone (Narcan) available at all times.
Pharmacy Cost & U.S. Healthcare Access
- Fentanyl: $60 - $150 per month for generic patches.
- Methadone: $10 - $25 per month for generic tablets.
- Insurance: Methadone is heavily preferred by Medicare and Medicaid on cost.
Clinical Decision Flow: Which Should You Choose?
Summary of the U.S. Clinical Choice Algorithm:
- Choose Fentanyl: If patient has heart issues, prefers patches, or has terminal cancer.
- Choose Methadone: If patient has nerve pain, high tolerance, or limited finances.
U.S. Clinical Decision Tree
Frequently Asked Questions
Yes, but avoid extreme heat like hot showers or saunas, which can cause overdosing.
Because it blocks NMDA receptors, which are the main switches for neuropathic signals.
Most U.S. insurance requires 'Prior Authorization' for Fentanyl patches due to cost.
In the opioid category, it is among the strongest medications safely used in American medicine.
Yes, it is more commonly associated with changes in metabolism than Fentanyl.