Fentanyl vs Morphine: Clinical Comparison, Potency & Side Effects
Fentanyl and Morphine are the two most historically significant opioids in American clinical history. While Morphine is the natural standard against which all other pain meds are measured, Fentanyl represents the absolute peak of synthetic opioid engineering.
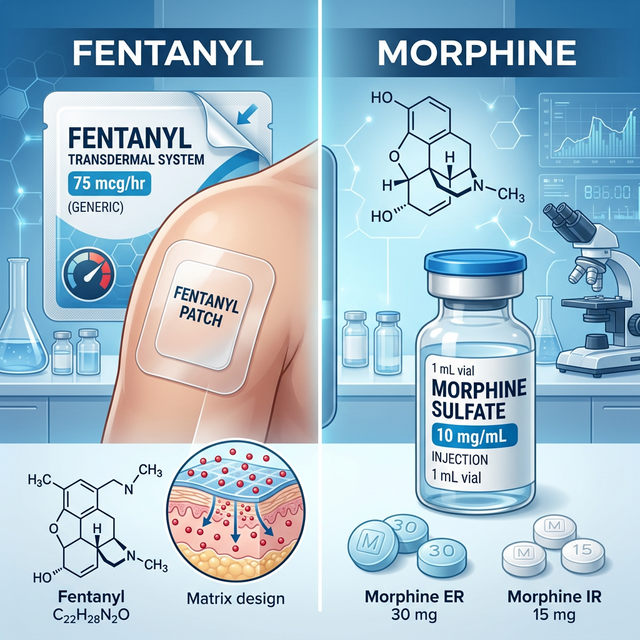
- Fentanyl: A purely synthetic molecule, approximately 100x stronger than morphine.
- Morphine (MS Contin): A natural alkaloid derived from the opium poppy; used as the 'baseline' (1.0) for MME calculations.
Choosing between them involves a trade-off between the 'tried-and-true' natural safety profile of Morphine and the advanced, fat-soluble efficiency of Fentanyl.

Dr. Kelsey Hopkins, MD
Dr. Hopkins practices rural family medicine in Southern Illinois, with a focus on community healthcare and chronic pain management.
Quick Reference Comparison
| Clinical Feature | Fentanyl | Morphine |
|---|---|---|
| U.S. Potency (Baseline) | 100.0 (Extreme) | 1.0 (The Standard) |
| Drug Class | Pure Synthetic Phenylpiperidine | Natural Opium Alkaloid |
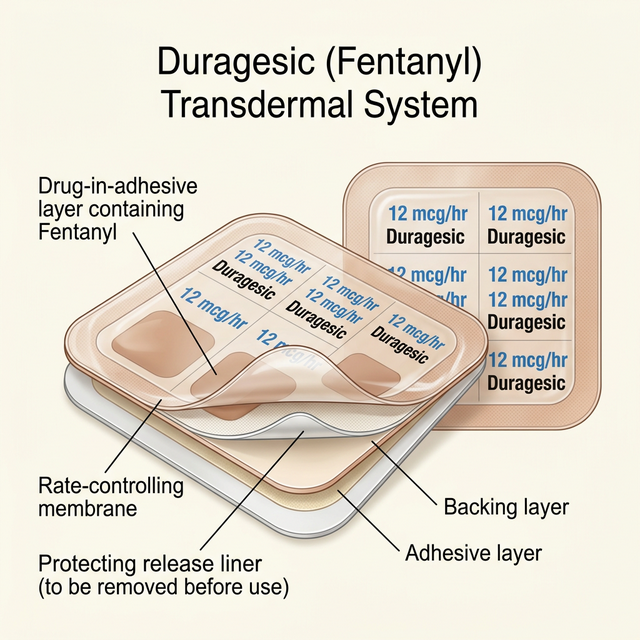
| Common U.S. Form | Transdermal Patch (72-hr) | Oral ER Tablet, Liquid, IV |
| Itching (Histamine) | Very Low | Extreme / High |
| DEA Schedule | Schedule II | Schedule II |
Clinical Profile: Fentanyl
Fentanyl is a highly fat-soluble opioid typically used for chronic, end-stage pain in the USA. Key details:
- Continuous Relief: Usually delivered via a 72-hour patch for stable, 'hands-free' pain control.
- No Bio-Transformation: Unlike codeine, it does not need to be converted by the liver to work.
- Low Volume: Clinical efficiency is high; tiny doses (mcg) provide massive relief.
It is the drug of choice for patients who have failing kidneys or severe itching from natural opioids.
Clinical Profile: Morphine

Morphine is known by U.S. brand names like MS Contin and Kadian. In the American market, it is valued for:
- The MME Standard: Every other opioid in the USA is measured in 'Morphine Milligram Equivalents'.
- Palliative Gold Standard: Still the most widely used medication for end-of-life comfort in hospitals.
- Metabolic Predictability: Doctors have over 100 years of data on how Morphine behaves in the human body.
While effective, it carries a higher risk of side effects like itching and nausea compared to Fentanyl.
Mechanism of Action: How They Work
How these drugs interact with American patients at the molecular level:
- Fentanyl: A purely synthetic 'key' that fits perfectly into Mu-Opioid receptors without any 'messy' side-targeting.
- Morphine: A natural 'key' that fits Mu-receptors but also triggers histamine release from mast cells.
- Biological Focus: Fentanyl treats pain with a 'surgical' strike; Morphine has a broader biological footprint.
Synthetic Power vs. Natural Standard
Lipid Entry
Fentanyl enters brain tissues 100x faster than Morphine pills.
Histamine Burst
Morphine triggers itching; Fentanyl rarely does.
MME Comparison
1mg Fentanyl = 100mg Morphine (Standard conversion).
Route Stability
Fentanyl patches bypass the 'peaks and valleys' of Morphine pills.
FDA-Approved vs. Off-Label Uses
FDA oversight and common U.S. clinical use:
- Fentanyl FDA: Persistent, severe chronic pain in patients already on 60mg MME/day.
- Morphine FDA: Moderate to severe pain where around-the-clock relief is needed.
- U.S. Hospital Use: Morphine is the first choice for chest pain during a heart attack (due to its ability to dilate blood vessels).
Potency and Clinical Strength
Potency comparison based on MME (Morphine Milligram Equivalents):
- Fentanyl (100x): The extreme peak of narcotic potency in American medicine.
- Morphine (1x): The mathematical constant used to weigh all other narcotics.
- Dosage Difference: A dose of Morphine is measured in milligrams (mg); Fentanyl is measured in thousands of times smaller micrograms (mcg).
Bioavailability & Metabolism
- Fentanyl: 92% bioavailability via patch; bypasses the liver's first-pass effect.
- Morphine: Low bioavailability (20-40%) when swallowed, as the liver destroys 60%+ before it enters the blood.
- Organ Safety: Morphine creates 'Active Metabolites' (M6G/M3G) that can build up in failed kidneys.
Half-Life & Duration of Action
- Fentanyl: Provides 72-hour steady-state coverage via the skin.
- Morphine ER: Provides 12-hour coverage; usually requires dosing twice daily.
- Morphine IR: Short duration (4 hours); used for breakthrough 'spikes' in pain.
Clinical Efficacy and Indications
Effectiveness in U.S. patient populations:
- Hospice/Palliative: Both are high-performing, but Morphine is easier to titrate in liquid form.
- Chronic Malignancy: Fentanyl is superior for its 'set-it-and-forget-it' patch convenience.
- Emergency ER Pain: Morphine is the standard IV choice for non-tolerant patients.
Typical Dosage and Administration
- Morphine ER: 15mg, 30mg, 60mg, 100mg, 200mg capsules.
- Fentanyl Patch: 12mcg, 25mcg, 50mcg, 75mcg, 100mcg per hour.
- Renal Protocol: Morphine doses MUST be reduced if kidney labs (creatinine) are abnormal.
Side Effects and Adverse Reactions
Common adverse reactions in American clinics:
- Histamine Release: Morphine causes significant itching, redness, and flushing.
- Sedation: Both cause sleepiness; Fentanyl is more likely to cause profound 'nodding'.
- Breathing: Fentanyl carries a higher risk of fatal respiratory arrest per milligram.
Comprehensive Side Effect Analysis
| Adverse Event | Fentanyl (Synthetic) | Morphine (Natural) |
|---|---|---|
| Nausea / Vomiting | High | Very High |
| Itching (Pruritus) | Low | Extremely High |
| Constipation | Very High | High |
| Kidney Metabolite Risk | Low | Extremely High |
| Respiratory Depression | Extreme | Severe |
🔴 Fentanyl Risks
- Severe drowsiness/sedation
- Nausea and vomiting
- Shallow, slow breathing
- Severe opioid-induced constipation
- Confusion in the elderly
🔴 Morphine Risks
- Moderate to severe itching
- Flushing or redness of the skin
- Nausea and stomach upset
- Dizziness when standing up
- Vivid hallucinations (in high doses)
⚠ Critical Safety Note
Serious adverse reactions require immediate medical attention. The following are life-threatening signs:
- Fatal respiratory depression
- Sudden hypotension (Blood pressure crash)
- Heat-induced Fentanyl overdose
- Myoclonus (Involuntary muscle jerks - Morphine)
- Coma
Safety, Addiction Risk, and Controlled Status
⚠ U.S. Regulation: EXTREME (USA SCHEDULE II)
Safety regulations and risks in American healthcare:
- The Kidney Rule: If your GFR is under 30, Morphine should be avoided to prevent neurotoxicity.
- The Patch Rule: Direct heat can make a Fentanyl patch lethal by overriding the 'slow release' gate.
- Abuse Potential: Both have an extremely high potential for dependence and withdrawal.
- Never use a heating pad or hot tub while wearing a Fentanyl patch.
- Morphine: Do not crush ER pills; it causes 'Dose Dumping'.
- Report any muscle twitching immediately if taking high-dose Morphine.
- Always keep Narcan (Naloxone) in the house of any opioid user.
Pharmacy Cost & U.S. Healthcare Access
- Morphine: Very affordable ($15-$40 per month via generic).
- Fentanyl: High-cost clinical medication ($60-$150).
- Hospice: Both are usually fully covered by Medicare Part D.
Clinical Decision Flow: Which Should You Choose?
Clinical decision tree for U.S. patients:
- Choose Morphine: For initial long-term pain control or patients who cannot wear patches.
- Choose Fentanyl: For patients with severe itching, kidney issues, or extremely high tolerance.
U.S. Opioid Selection Logic
Frequently Asked Questions
Yes. It is chemically structured to be 100x stronger and more fat-soluble than Morphine.
Natural opioids trigger the release of histamine from mast cells, whereas synthetic Fentanyl doesn't.
Occasionally, doctors prescribe liquid Morphine for 'breakthrough' pain while using a Fentanyl patch for baseline pain.
No, but it creates waste products that only kidneys can remove. If kidneys fail, these waste products become toxic.
Both are Schedule II narcotics with an extremely high risk of addiction and dependence.